Pain Patch for Upper Back Pain: Trapezius and Rhomboid Relief Guide
Evidence-based guide to pain patches for upper back pain. Compare menthol, lidocaine, and diclofenac patches, learn application areas, and combine with stretching and posture correction for trapezius and rhomboid pain.
Jun 22nd,202619 Views
Key Statistics:
Approximately 65% of adults report upper back pain (between the shoulder blades) at some point in their lives, often linked to prolonged sitting and poor posture.
The trapezius and rhomboid muscles are the most common sources of upper back tension and trigger-point pain in office workers and drivers.
Topical pain patches deliver medication 3-5x more concentrated at the site of pain than oral alternatives, with lower systemic exposure.
Randomized trials show diclofenac patches reduce upper back pain scores by 35-50% within 7 days versus placebo.
Lidocaine 4-5% patches can relieve myofascial trigger-point pain within 30 minutes, with effects lasting up to 12 hours per application.
Combining patches with posture correction and stretching reduces recurrence of upper back pain by up to 60% over 12 weeks.
TL;DR
Pain patches for upper back pain deliver menthol, lidocaine, diclofenac, or capsaicin directly to the trapezius and rhomboid muscles.
Best results come from matching the patch type to the pain pattern: menthol for acute tightness, lidocaine for sharp trigger points, diclofenac for inflammation-dominant pain.
Apply patches around-not directly on-the spine, over the belly of the trapezius or between the shoulder blade and spine.
Wear for 4-12 hours per application; do not exceed the duration stated on the label.
Patches work best as part of a posture correction + stretching program; they relieve pain but do not address the underlying muscle imbalance.
Key Takeaways
Trapezius & rhomboid pain: The two muscles most responsible for upper back tension, both reachable with topical patches.
Patch selection matters: Menthol, lidocaine, diclofenac, capsaicin, and herbal patches work through different mechanisms.
Application is local: Apply over the tender trigger point, never on broken skin or directly over the spine.
4-12 hour wear time: Most OTC patches are designed for one application per day or one every 12 hours.
Combine with movement: Stretching, ergonomic posture, and strengthening exercises prevent recurrence.
Know when to see a doctor: Sharp radiating pain, numbness, or pain after trauma requires medical evaluation.
Medically reviewed by the KONGDY Health Editorial Team. Last updated: 2026-06-22.
Quick Answer
Pain patches for upper back pain deliver active ingredients through the skin directly to the trapezius and rhomboid muscles. Menthol patches work best for acute muscle tightness, lidocaine patches for sharp trigger-point pain, and diclofenac patches for inflammation-dominant pain. Apply the patch over the tender area, smooth from the center outward, and wear for 4-12 hours as directed. Combine with posture correction and stretching for lasting relief.
Introduction
Upper back pain-between the shoulder blades and across the trapezius-is one of the most common complaints in modern desk-bound life. Unlike the lower back, which bears the brunt of lifting injuries, the upper back is more often a victim of posture: hours hunched over a keyboard, neck craned forward, shoulders rounded inward. Over weeks and months, this posture strains the trapezius and rhomboid muscles, creating trigger points that radiate pain across the shoulders and up into the neck.
Pain patches have become a frontline tool for upper back pain because they deliver medication directly to the affected muscles without the gastrointestinal side effects of oral NSAIDs. This guide draws on 36 years of topical patch development and current clinical evidence to explain how to choose, apply, and combine patches for the best results.
What Is Upper Back Pain?
The "upper back" refers to the thoracic region of the spine-T1 through T12-and the muscles that attach to it. Most upper back pain is myofascial (muscle and connective tissue), not joint or disc related. The three muscle groups most often involved are:
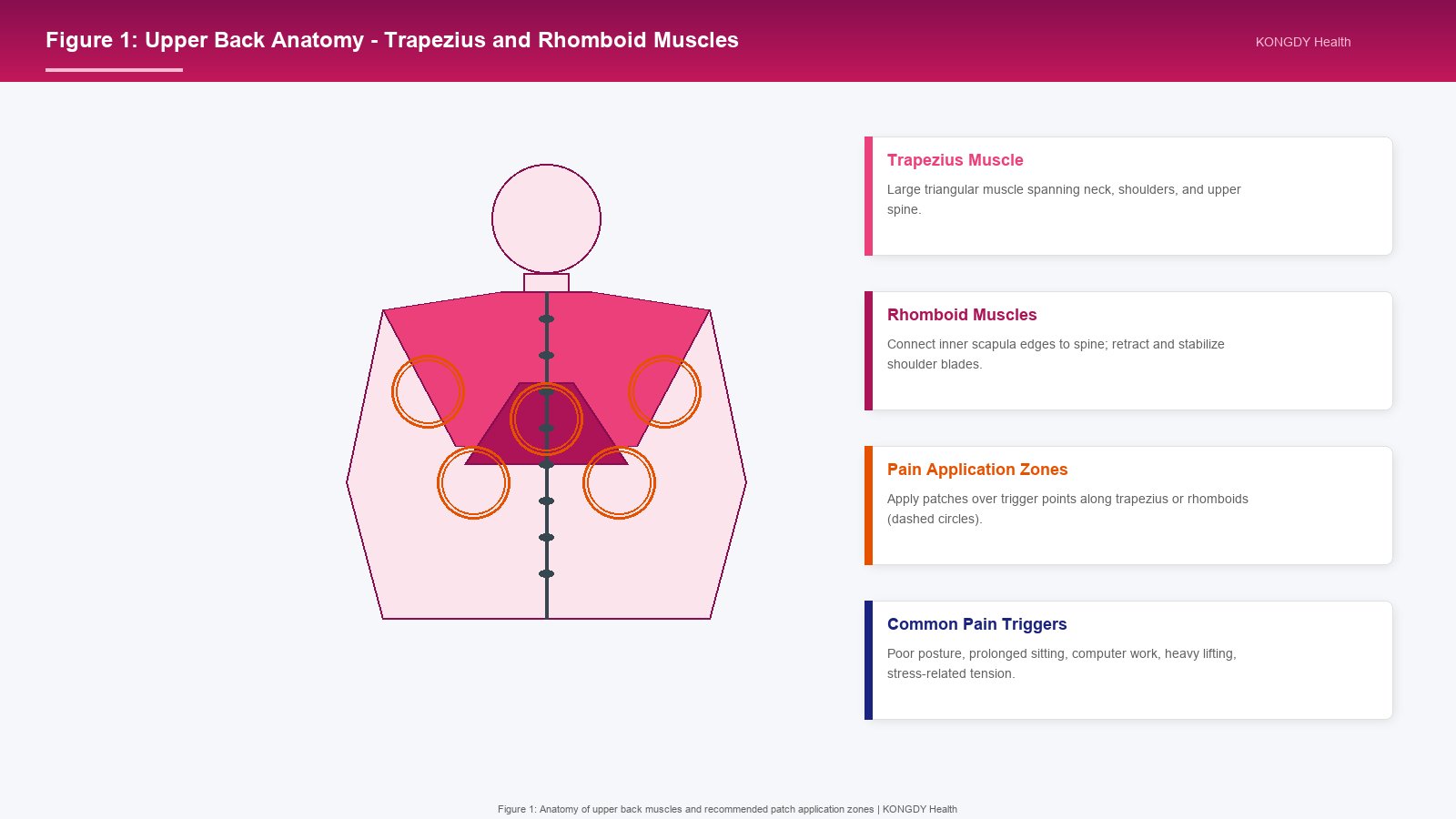
Trapezius: A large, triangular muscle running from the base of the skull and cervical spine down to the shoulder blades and mid-back. The upper fibers elevate the shoulders; the lower fibers depress them. Trigger points in the upper trapezius refer pain up the neck and into the temple.
Rhomboids: Two muscles (major and minor) that connect the inner edge of the shoulder blade to the spine. They retract the scapula and stabilize the shoulder girdle. Trigger points cause a deep, aching pain between the shoulder blades.
Levator scapulae: Connects the upper cervical spine to the top of the shoulder blade. Trigger points cause stiffness when turning the head and pain at the top of the shoulder.
Upper back pain differs from lower back pain in several important ways:
Disc herniation is rare in the thoracic spine because the rib cage stabilizes the vertebrae.
Nerve compression is uncommon; most upper back pain is muscular rather than neurological.
Posture is the dominant cause, followed by stress-related muscle tension, overuse, and trauma.
Common Causes of Upper Back Pain
Understanding the cause of your upper back pain helps you choose the right patch and the right complementary treatment. The most common causes include:
Poor posture: Forward head posture and rounded shoulders place sustained load on the trapezius and rhomboids. Hours of computer work, smartphone use, or driving create chronic tension.
Muscle overuse: Repetitive lifting, overhead reaching, or sustained shoulder elevation (e.g., painting, stocking shelves) overload the upper back muscles.
Stress and anxiety: Psychological stress causes chronic elevation of the shoulders and tightening of the trapezius, often without conscious awareness.
Trigger points: Myofascial trigger points are hyperirritable knots in the muscle that refer pain to a predictable area. They can be activated by acute strain, poor posture, or chronic overload.
Trauma: Whiplash, falls, or sports injuries can strain the upper back muscles and ligaments.
Sleep position: Sleeping on the stomach or with poor pillow support can strain the upper back and neck overnight.
Underlying conditions: In rare cases, upper back pain can signal thoracic disc herniation, vertebral compression fracture (especially in osteoporosis), or referred pain from cardiac or pulmonary conditions.
Figure 1: Anatomy of upper back muscles-trapezius and rhomboids-and the recommended patch application zones (dashed circles) for tension and trigger-point pain.
How Pain Patches Help Upper Back Pain
Pain patches deliver active ingredients through the skin directly to the underlying muscles. This topical route has several advantages over oral medications:
Concentrated delivery: Medication reaches the target tissue at higher local concentrations than oral dosing.
Reduced systemic exposure: Less medication circulates in the bloodstream, reducing the risk of gastrointestinal, hepatic, and renal side effects.
Sustained release: Most patches deliver medication over 4-12 hours, providing consistent pain relief.
Bypasses digestion: Useful for patients who cannot tolerate oral NSAIDs.
Easy to apply: No water, swallowing, or timing with meals required.
The five main types of patches used for upper back pain differ in their active ingredients and mechanisms of action.
Pain Patch Types for Upper Back Pain at a Glance
Patch Type
Active Ingredient
Strength
Relief Duration
Best For
Menthol
Menthol
3-10%
4-8 hours
Acute muscle tightness, cooling relief
Lidocaine
Lidocaine
4% OTC / 5% Rx
12 hours
Sharp trigger-point pain
Diclofenac
Diclofenac sodium
1-2%
12 hours
Inflammation-dominant pain
Capsaicin
Capsaicin
0.025-0.1%
8-12 hours
Chronic tension, long-term use
Herbal
Methyl salicylate, camphor, etc.
Varies
6-10 hours
Daily management, sensitive users
Menthol Patches
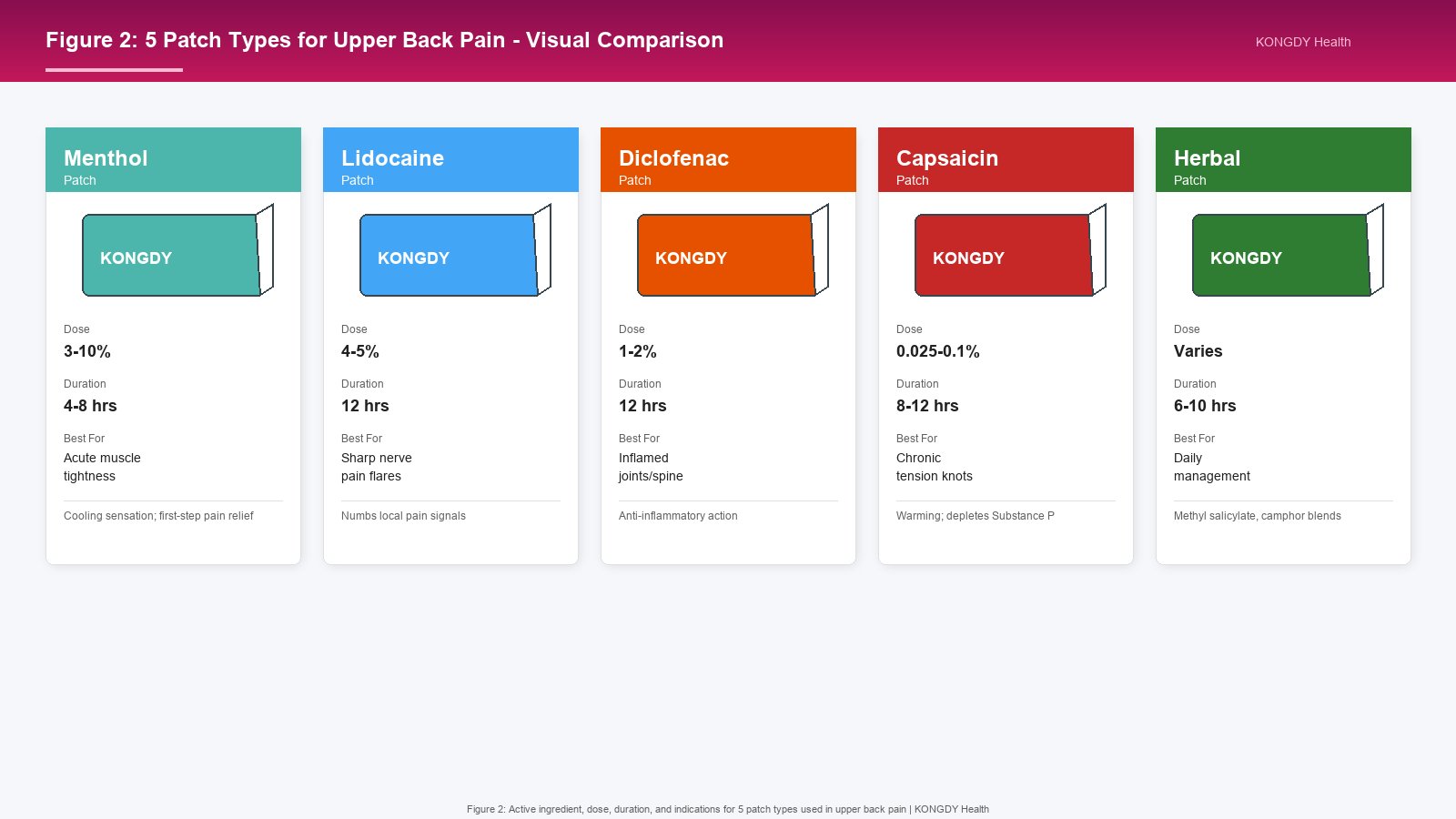
Menthol patches produce a cooling sensation that overrides pain signals through the gate-control mechanism. They are first-line for acute muscle tightness in the upper back. Effects begin within minutes and last 4-8 hours. Menthol patches are widely available OTC and are safe for most adults. They do not reduce inflammation but provide effective symptomatic relief.
Lidocaine Patches
Lidocaine is a local anesthetic that blocks sodium channels in nerve fibers, numbing the area where it is applied. OTC 4% lidocaine patches are available in many countries; 5% prescription patches are used for post-herpetic neuralgia and other neuropathic conditions. For upper back trigger points, lidocaine provides rapid, targeted numbness within 30 minutes. Each application lasts up to 12 hours.
Diclofenac Patches
Diclofenac is a nonsteroidal anti-inflammatory drug (NSAID). Diclofenac patches deliver the medication directly to the inflamed tissue, with less gastric side-effect risk than oral diclofenac. Clinical trials show 35-50% pain score reductions in upper back and neck pain over 7-14 days. They are ideal when inflammation is the dominant pain driver, such as after acute strain.
Capsaicin Patches
Capsaicin-the compound that makes chili peppers hot-depletes Substance P, a neurotransmitter involved in pain signaling. Capsaicin patches produce a warming sensation followed by sustained pain relief. Effects build over several days of repeated use. They are well suited to chronic upper back tension but can cause skin irritation in sensitive users.
Herbal and Combination Patches
Herbal patches contain methyl salicylate, camphor, eucalyptus oil, and other plant-derived ingredients. They produce mild warming or cooling sensations and are popular for daily management. Combination patches often layer menthol, methyl salicylate, and camphor to provide both cooling and warming sensations.
Figure 2: Comparison of 5 patch types for upper back pain-menthol, lidocaine, diclofenac, capsaicin, and herbal-with dose, wear time, and best-use indications.
Best Patch Types for Specific Upper Back Conditions
For Acute Tension and Tightness
Acute upper back tension-from long desk sessions or stress-usually responds well to menthol or herbal patches. The cooling or warming sensation provides immediate relief while the underlying muscles recover. Apply as soon as you notice tension building; do not wait for full-blown pain.
For Trigger-Point Pain
Trigger points are localized, hyperirritable knots that refer pain in a predictable pattern. Lidocaine 4-5% patches are highly effective for trigger points because they directly numb the nerve fibers transmitting the pain signal. Apply the patch directly over the most tender spot; relief should begin within 30 minutes.
For Post-Injury Inflammation
After an acute strain, lifting injury, or sports-related upper back pain, diclofenac patches address the underlying inflammation. They are most effective when started within 48-72 hours of the injury and used consistently for 7-14 days.
For Chronic Tension
Chronic upper back tension-of months or years duration-responds best to capsaicin patches used daily for several weeks. The gradual depletion of Substance P reduces the overall sensitivity of the upper back to pain.
For Sensitive Skin
Users with sensitive skin or allergies to adhesives may tolerate herbal patches better than menthol, capsaicin, or lidocaine. Look for hypoallergenic adhesive and fragrance-free formulations.
Where to Apply a Pain Patch for Upper Back Pain
Correct application is critical. Follow these principles:
Apply over the tender area: Feel for the tightest, most painful spot in the trapezius or rhomboid area. That is where the patch should go.
Avoid the spine: Do not place patches directly over the spinous processes. Apply 2-3 cm (about 1 inch) to either side, over the belly of the muscle.
Between the shoulder blades: For mid-back pain, place the patch over the rhomboid area between the spine and the inner edge of the shoulder blade.
Upper trapezius: For neck and shoulder tension, place the patch at the top of the shoulder, halfway between the base of the neck and the shoulder joint.
Avoid broken skin: Never apply a patch over cuts, scrapes, sunburn, or irritated skin.
Avoid moles and birthmarks: Skin lesions can react unpredictably to topical medication.
Common Application Zones
Upper trapezius (both sides): Top of the shoulder, 3-5 cm lateral to the cervical spine. Target: chronic shoulder tension.
Mid-trapezius: Midway between the shoulder blade and the spine, at the level of the shoulder. Target: desk-work tension.
Rhomboid area (both sides): Between the inner border of the shoulder blade and the spine. Target: deep aching between the shoulder blades.
Levator scapulae: At the top of the shoulder blade, near the base of the neck. Target: stiffness when turning the head.
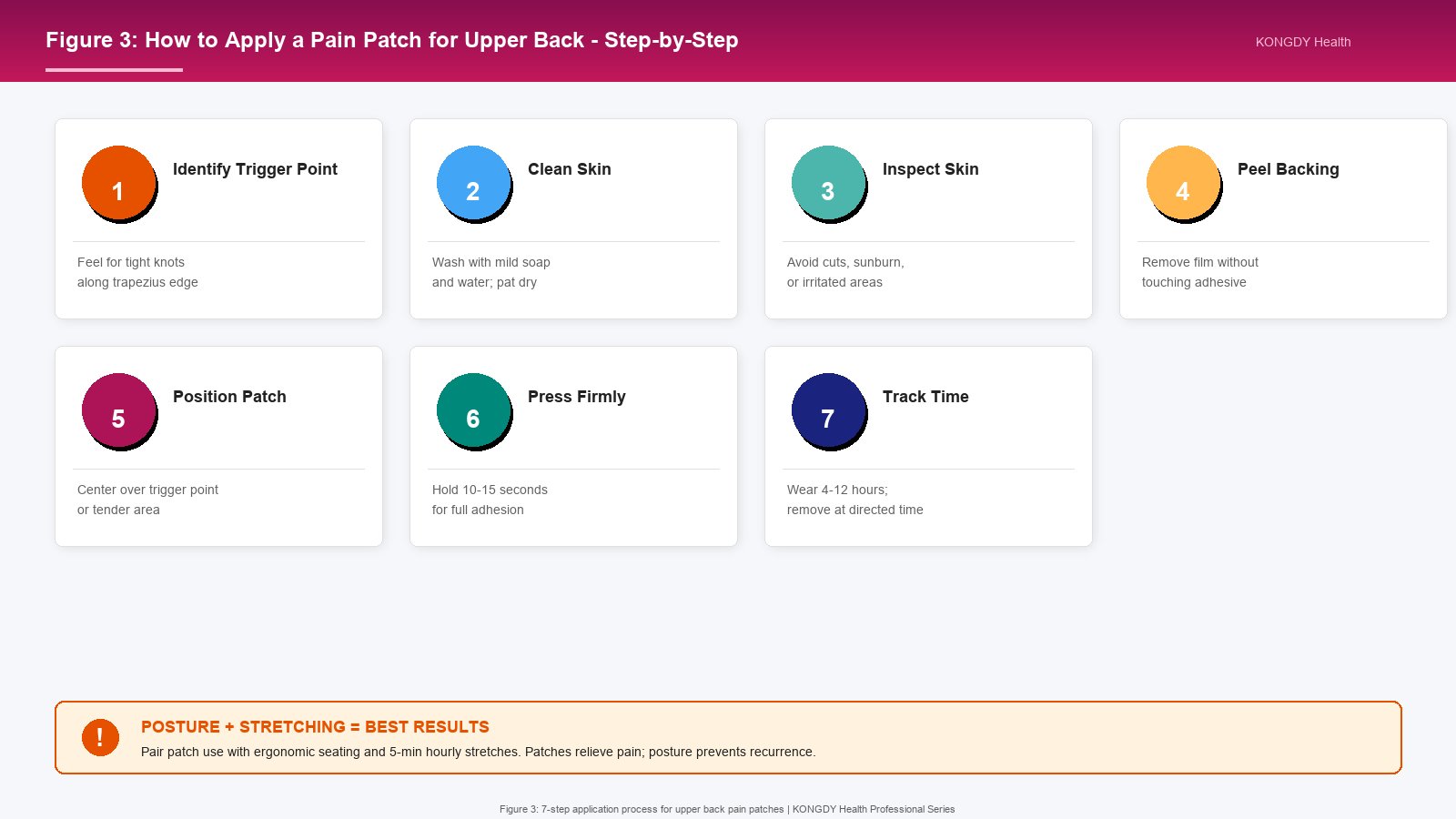
Figure 3: 7-step application process for upper back pain patches, from identifying trigger points to tracking wear time and combining with posture correction.
How to Apply a Pain Patch for Upper Back Pain: Step-by-Step
Identify the trigger point: Use your fingers to feel for the tightest, most tender spot in the trapezius or rhomboid area. Press gently and note where the pain is most intense.
Clean the skin: Wash the application area with mild soap and water. Pat dry thoroughly. Avoid alcohol-based cleansers, which can irritate the skin under the patch.
Inspect the skin: Make sure the area is free of cuts, sunburn, rashes, moles, or irritation. If any of these are present, choose a different application site.
Peel the backing: Remove the protective film without touching the adhesive surface. Oils from your fingers can reduce adhesion.
Position the patch: Center the patch over the trigger point or tender area, 2-3 cm lateral to the spine if applying near the mid-back.
Press firmly: Smooth the patch from the center outward, pressing for 10-15 seconds to ensure full adhesion. The patch should lie flat without wrinkles or air bubbles.
Wash hands and track time: Wash your hands after application to remove any residual medication. Note the time you applied the patch and remove it at the directed interval (typically 4-12 hours).
Application Best Practices
To get the most from your upper back pain patch:
Rotate sites: If you use patches daily, alternate between slightly different locations to prevent skin irritation.
Do not overlap patches: Do not place two patches on top of each other. The medication absorption profile is calibrated for single-patch use.
Time it right: Apply at the onset of pain or before activities that trigger pain (e.g., before a long drive).
Do not shower immediately after: Wait at least 30 minutes after removing a patch before showering, to allow the skin to recover.
Watch for skin reactions: Remove the patch immediately if you develop redness, itching, or rash. Most reactions are mild and resolve within hours.
Combine with movement: Apply the patch, then perform gentle stretching or posture correction exercises. The medication makes movement easier; movement accelerates recovery.
Common Mistakes to Avoid
Applying over clothing: Patches must contact skin directly. Adhesion and absorption are impaired over fabric.
Applying to wet or oily skin: Dry the area thoroughly before application.
Cutting patches: Cutting a patch can disrupt the medication distribution. Use a smaller patch instead.
Re-using single-use patches: Single-use patches lose their medication after the first wear.
Wearing longer than directed: Prolonged wear does not increase benefit and increases the risk of skin irritation.
Combining Pain Patches with Other Treatments
Patches work best as part of a comprehensive plan. The most effective combinations for upper back pain include:
Heat therapy: Applying a warm compress or heating pad for 15-20 minutes before or after a patch can relax muscles and improve absorption. Do not apply heat over a patch.
Cold therapy: Ice packs reduce acute inflammation. Use ice for 15 minutes, then wait at least 30 minutes before applying a patch.
Stretching: Gentle upper back stretches-chest openers, scapular squeezes, cat-cow-improves range of motion and reduces trigger point activity.
Posture correction: Ergonomic chair setup, monitor at eye level, and frequent breaks prevent the recurrence of upper back tension.
Strengthening exercises: Strengthening the rhomboids, lower trapezius, and rotator cuff muscles provides long-term stability.
Massage: Self-massage or professional massage therapy can deactivate trigger points. Patches provide relief between sessions.
Oral medications: For severe pain, oral NSAIDs or acetaminophen can be combined with topical patches. Consult a doctor before combining treatments.
Recovery Timeline for Upper Back Pain
Most upper back pain improves significantly within 2-6 weeks of consistent treatment. A typical recovery timeline looks like this:
Days 1-3: Acute pain phase. Use ice for the first 48-72 hours if inflammation is present; switch to heat thereafter. Apply patches as directed for pain relief.
Days 4-7: Subacute phase. Begin gentle stretching and posture correction. Continue patch use, particularly before activities that aggravate pain.
Weeks 2-3: Recovery phase. Gradually introduce strengthening exercises. Reduce patch use as pain subsides; do not stop abruptly if pain persists.
Weeks 4-6: Maintenance phase. Continue posture correction and a regular stretching/strengthening routine. Use patches as needed for flare-ups.
Weeks 6+: Most acute upper back pain should be resolved by this point. If pain persists beyond 6 weeks, consult a healthcare provider.
When to See a Doctor
Most upper back pain is muscular and responds to self-care. However, certain symptoms require medical evaluation:
Pain after trauma: A fall, car accident, or sports injury warrants medical evaluation to rule out fracture or serious soft-tissue damage.
Sharp, radiating pain: Pain that shoots down the arm, into the chest, or around the ribs may indicate nerve involvement.
Numbness or tingling: Numbness or weakness in the arms or hands suggests cervical nerve compression.
Pain that worsens at night: Night pain that disrupts sleep may indicate a more serious underlying condition.
Fever, weight loss, or fatigue: Systemic symptoms alongside upper back pain require prompt medical attention.
Pain lasting more than 6 weeks: Persistent pain despite self-care should be evaluated by a healthcare provider.
Difficulty breathing or chest pain: Severe chest pain or shortness of breath may indicate cardiac or pulmonary conditions; seek emergency care.
Prevention Strategies for Upper Back Pain
Preventing recurrence is as important as treating acute pain. The most effective prevention strategies include:
Ergonomic workstation: Position your monitor at eye level, your keyboard at elbow height, and your chair so your feet are flat on the floor.
Frequent breaks: Stand and stretch every 30-60 minutes during desk work. A 2-minute break every hour dramatically reduces upper back strain.
Strengthening exercises: Target the rhomboids, lower trapezius, and rotator cuff. Strong postural muscles prevent the forward-rounded posture that drives upper back pain.
Stress management: Stress-related shoulder tension responds to mindfulness, breathing exercises, and regular physical activity.
Sleep posture: Sleep on your back or side with a pillow that supports the natural curve of your neck. Avoid sleeping on your stomach.
Hydration: Adequate hydration supports muscle and connective tissue health.
Appropriate lifting: Lift with your legs, not your back. Avoid lifting heavy objects overhead; use a step stool when needed.
Daily Habits for a Healthy Upper Back
Small daily habits add up to long-term upper back health:
Scapular squeezes: 10 reps, 3 times per day
Chin tucks: 10 reps, 3 times per day
Doorway chest stretches: 30 seconds, twice daily
Walking: 30 minutes most days of the week
Hydration: 2-3 liters of water daily
Frequently Asked Questions
1. Which pain patch is best for upper back pain?
The best patch depends on the type of pain. Menthol patches are best for acute muscle tightness and first-step pain relief. Lidocaine patches work well for sharp trigger-point pain. Diclofenac patches address inflammation-dominant pain. Capsaicin patches suit chronic tension. Herbal patches are appropriate for daily management and sensitive users. Many people keep two types on hand: menthol for acute relief and lidocaine or diclofenac for flare-ups.
2. Where should I apply a pain patch for upper back pain?
Apply the patch over the most tender area in the trapezius or rhomboid region. Avoid placing patches directly over the spine; instead, apply 2-3 cm (about 1 inch) to either side, over the belly of the muscle. Common application zones include the upper trapezius (top of the shoulder), mid-trapezius (mid-back near the shoulder blade), and the rhomboid area (between the spine and shoulder blade). Avoid broken skin, moles, and irritated areas.
3. How long should I use pain patches for upper back pain?
Most OTC patches are designed for 4-12 hours per application, with one to two applications per day. For acute pain, use patches as needed for 1-2 weeks. For chronic conditions, longer-term use under medical supervision may be appropriate. Do not exceed the duration stated on the label. If pain persists beyond 6 weeks of consistent patch use and self-care, consult a healthcare provider.
4. Can pain patches cure upper back pain?
Pain patches do not cure the underlying cause of upper back pain; they relieve symptoms. To address the root cause, combine patches with posture correction, stretching, strengthening exercises, and ergonomic improvements. Most upper back pain is caused by chronic muscle imbalance and poor posture; patches provide relief while you address these underlying factors.
5. Are pain patches safe with other upper back pain treatments?
Most patches can be safely combined with heat, cold, stretching, massage, and posture correction. For oral medications, patches have fewer interactions than oral NSAIDs because of their localized action. Consult your doctor before combining patches with oral pain medications, especially if you take blood thinners, blood pressure medications, or other chronic medications.
6. Can I use pain patches with oral medications?
Yes, in most cases, topical patches can be combined with oral pain relievers. However, if you are taking oral NSAIDs (ibuprofen, naproxen, diclofenac), combining with a diclofenac patch may increase total NSAID exposure. Consult your doctor or pharmacist before combining, especially if you have a history of ulcers, kidney disease, or bleeding disorders.
7. When should I see a doctor for upper back pain?
See a doctor if your pain follows trauma, radiates into the arm or chest, is accompanied by numbness or weakness, worsens at night, or persists despite 6 weeks of self-care. Also seek medical attention if you experience fever, unexplained weight loss, or shortness of breath alongside upper back pain. These symptoms may indicate conditions that require specific treatment.
8. Can pain patches be used during pregnancy or for children?
Menthol and herbal patches are generally considered safe during pregnancy, but diclofenac and lidocaine patches should be avoided unless specifically prescribed by a physician. Capsaicin patches can cause skin irritation and are usually not recommended during pregnancy. For children, follow age guidelines on the label-typically age 12+ for most OTC patches-and consult a pediatrician for younger children.
9. How do I know if my pain patch is working?
You should notice pain relief within 30 minutes for menthol and lidocaine patches, and within several hours for diclofenac patches. Capsaicin patches may take several days of consistent use to show full effect. If you notice no improvement after the recommended initial period, consider switching to a different patch type or consulting a healthcare provider. Some people respond better to certain active ingredients than others.
10. What's the difference between menthol and diclofenac patches for upper back pain?
Menthol patches provide sensory relief-a cooling sensation that overrides pain signals without reducing inflammation. They are best for muscle tightness and acute discomfort. Diclofenac patches are anti-inflammatory-they reduce the underlying inflammation that contributes to pain, making them ideal for post-injury or inflammation-dominant upper back pain. Many people use menthol for daily management and diclofenac for flare-ups.
Quick Reference: Pain Patch Selection for Upper Back Pain
Depletes Substance P over weeks; long-term management
Daily maintenance; sensitive skin
Herbal (menthol + methyl salicylate)
Mild, fragrance-light options for regular use
Pain before bed to improve sleep
Menthol or lidocaine
Calms the area; reduces night-time discomfort
Pain before physical activity
Menthol or diclofenac
Pre-emptive relief; easier movement during exercise
Combined with oral NSAIDs
Lidocaine or menthol
Avoids NSAID stacking; uses different mechanism
Stress-related shoulder tension
Menthol or warming herbal
Sensory distraction; relaxation cue
Children age 12+ or pregnancy (consult MD)
Menthol or herbal only
Lower systemic absorption; safer profile
About KONGDY Health
KONGDY Health is a leading manufacturer of pain relief patches with 36 years of expertise in transdermal patch technology. Our portfolio includes menthol, lidocaine, diclofenac, capsaicin, and herbal patch formulations for OEM and private-label customers worldwide. We hold ISO 13485, CE, and FDA certifications, and serve distributors, pharmacies, and brand owners across 60+ countries.
Whether you are launching a new pain patch line or expanding an existing catalog, our team can help with custom formulation, packaging design, regulatory support, and bulk manufacturing. Contact KONGDY Health to discuss your requirements or explore our pain patch catalog.